Radical change will be needed in order to save lives from the drug overdose pandemic
The provisional drug overdose death statistics for 2020 confirmed the addiction field’s worst fears.
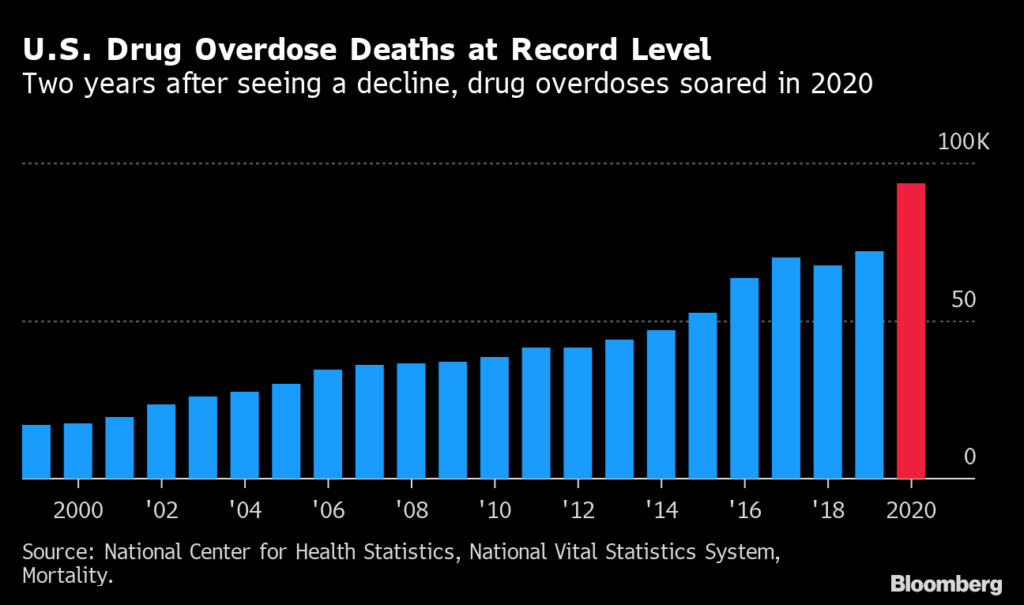
More people died of overdoses in the United States last year than in any other one-year period in our history. More than 93,000 people died. The increase from the previous year was also more than we’ve ever seen—up 30 percent.
These data are telling us that something is wrong. In fact, they are shouting for change.
It is no longer a question of “doing more” to combat our nation’s drug problems. What we as a society are doing—putting people with drug addiction behind bars, underinvesting in prevention and compassionate medical care—is not working. Even as we work to create better scientific solutions to this crisis, it is beyond frustrating—it is tragic—to see the effective prevention and treatment tools we already have just not being used.
The benefits of providing effective substance use disorder treatments—especially medication for opioid use disorder—are well-known. Yet decades of prejudice against treating substance use disorders with medication has greatly limited their reach, partly accounting for why only 18 percent of people with opioid use disorder receive medications. Historical reluctance to provide these treatments and of insurers to cover them reflects the stigma that has long made people with addiction a low priority.
We must eliminate the attitudes and infrastructure barring treating people with substance use disorders. This means making it easier for clinicians to provide life-saving medications, expanding models of care like digital health technologies and mobile clinics that can reach people where they are, and ensuring that payers cover treatments that work.
The science of the matter is unequivocal: Addiction is a chronic and treatable medical condition, not a weakness of will or character or a form of social deviance. But stigma and longstanding prejudices—even within healthcare—lead decision-makers across healthcare, criminal justice, and other systems to punish people who use drugs rather than treat them. That approach may be simpler than asking us as a society to have compassion or care for people with a devastating, debilitating, often fatal disorder. But the risk of incarceration does not deter drug use, let alone address addiction; it perpetuates stigma, and disproportionately harms the most vulnerable communities.
Evidence-based harm reduction, such as syringe services programs, also need to be a part of any solution to our drug crisis, as these have been shown to reduce HIV and hepatitis C transmission, and help link people to treatment for addiction and other conditions. While the federal government has embraced evidence-based harm-reduction programs, many communities continue to resist them, erroneously thinking they sanction or encourage drug use. Multiple independent studies have shown that they don’t. Researchers are also evaluating innovative but historically controversial strategies operating abroad like overdose prevention centers, where people can use substances under medical supervision and access other health services, to evaluate cost-effectiveness and ability to reduce deaths and improve health.
Part of the failure of the current approach to the drug crisis arises from the unrealistic expectation that people should—and can—just stop using drugs. Little concern is shown for people with addiction unless and until they are drug-free, but the reality is that difficulties and resumed use typically mark the recovery journey. Compassion, care, and support need to extend to those still using drugs and those who return to drug use, not just to those who can satisfy the stringent standards of abstinence. Everyone with a substance use disorder, regardless of whether they are currently using drugs, needs good healthcare and may also need help with housing, employment, and childcare needs.
To prevent young people from misusing drugs and to keep people from all ages from developing substance use disorders, our nation must address the social and economic stressors that increase the risk of drug use, such as poverty and housing instability, unsafe neighborhoods and schools, and other effects of a changing economy including social isolation and despair. Drug overdose deaths are one component of the “deaths of despair” that, along with suicide and alcohol-related illness, have caused life expectancy to decline in the U.S., even before the 1.5-year drop in 2020 caused largely by the COVID-19 pandemic.
On the ground, evidence-based interventions can make a big difference: Universal prevention programs as well as interventions targeted to the most at-risk families and youth not only reduce the risk of later drug taking and addiction but have radiating benefits on other aspects of mental and physical health.
This poses a question of collective willingness to invest in these measures. The long-term savings in healthcare and justice costs relative to the costs of prevention interventions can be substantial. But they are long-term investments with benefits that will take time to accrue, and the nature of our society is to look at short-term bottom lines and expect immediate results. Read more from SA